Breast Cancer
Background:
Breast cancer is the most frequently diagnosed life-threatening cancer in women. It is the leading cause of cancer death among women.
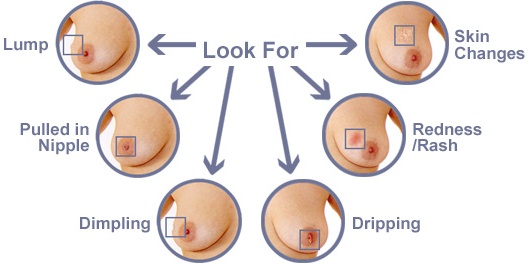
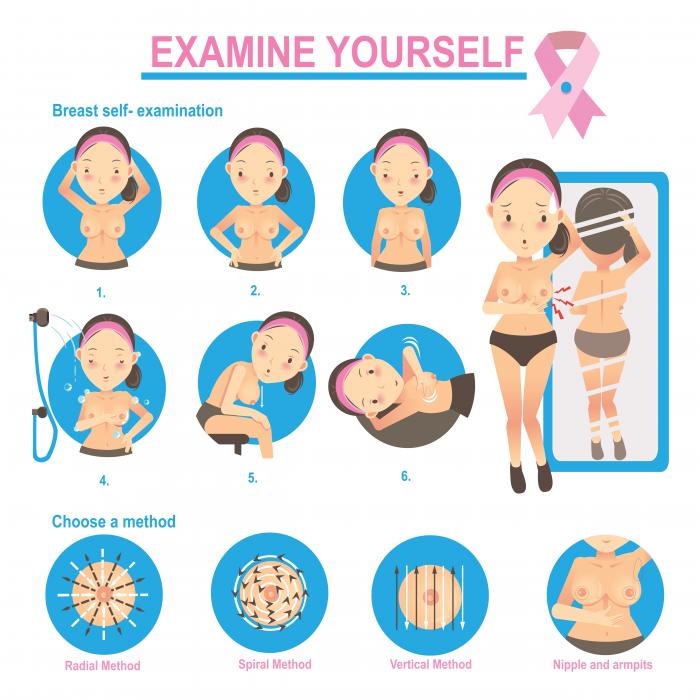
Many early breast carcinomas may be asymptomatic; pain or discomfort is not usually a symptom of breast cancer. Breast cancer is often first detected as an abnormality on a mammogram before the patient or healthcare provider feels it.
Increased public awareness and improved screening have led to earlier diagnosis, at stages amenable to complete surgical resection and curative therapies. Consequently, survival rates for breast cancer have improved significantly, particularly in younger women.
Surgery is considered primary treatment for breast cancer. Many patients with early-stage breast cancer are cured with surgery alone.

Treatment
Surgery is considered primary treatment for breast cancer, as many patients with early-stage disease are cured with surgery alone. The goals of breast cancer surgery include complete resection of the primary tumor with negative margins to reduce the risk of local recurrences, and pathologic staging of the tumor and axillary lymph nodes for providing necessary prognostic information. Several different types of operations are available for the treatment of breast cancer.
Adjuvant treatment for breast cancer involves radiation therapy and a variety of chemotherapeutic and biologic agents.

Prognosis
Numerous prognostic and predictive factors for breast cancer have been identified by the College of American Pathologists (CAP) to guide the clinical management of women with breast cancer.
Breast cancer prognostic factors include the following:
- Axillary lymph node status
- Tumor size
- Lymphatic/vascular invasion
- Patient age
- Histologic grade
- Histologic subtypes (eg, tubular, mucinous [colloid], papillary)
- Response to neoadjuvant therapy
- ER/ PR status
- HER2 gene amplification and/or overexpression
Breast cancer predictive factors include the following:
- ER/PR status
- HER2 gene amplification and/or overexpression
Cancerous involvement of the lymph nodes in the axilla is an indication of the likelihood that the breast cancer has spread to other organs. Survival and recurrence are independent of level of involvement but directly related to the number of involved nodes.
Patients with node-negative disease have an overall 10-year survival rate of 70% and a 5-year recurrence rate of 19%. In patients with lymph nodes that are positive for cancer, the recurrence rates at 5 years are higher (30-70%)
Hormone-positive tumors have a more indolent course and are responsive to hormone therapy.
Five-year survival rates are highly correlated with tumor stage, as follows:
- Stage 0: 99-100%
- Stage I: 95-100%
- Stage II: 86%
- Stage III: 57%
- Stage IV: 20%
This prognostic information can guide physicians in making therapeutic decisions. Pathologic review of the tumour tissue for a histological grade along with the determination of estrogen/progesterone receptor status and HER2 status is necessary for determining prognosis. Evaluation of lymph node involvement by sentinel lymph node biopsy or axillary lymph node dissection is generally necessary as well.